
One year ago today the World Health Organization (WHO) declared that COVID-19 was a pandemic. Twelve months on, one can be forgiven for forgetting what life without COVID-19 looks like. But cooped-up Europeans receive occasional reminders, thanks to images circulating on social media of young people partying in Wuhan, the Chinese city where the virus is thought to have originated, or of massive crowds packing out sports stadiums in New Zealand.
It would have been nice to be in the same place. In principle, Great Britain, as an island, could have implemented the same suite of ‘zero-COVID’ policies that are responsible for such outcomes: a rapid and effective lockdown, with comprehensive financial support, effective test-and-tracing, and what epidemiologist Professor Devi Sridhar calls “very tight border restrictions”. (The United Kingdom, with its land border to the EU via Ireland, presents a tougher challenge, although not one that has received the attention it deserves.)
Our government failed entirely on every single one of these, and the result has been to leave us as a global leader in death and infection. Tens of thousands of people died unnecessarily because of last year’s government failure.
This has led many to demand that the UK should now change course and adopt the zero-COVID approach to tackling the pandemic, learning from best practice elsewhere. Combined with the successful national vaccine rollout, its protagonists claim that a zero-COVID strategy would, if applied and held to, allow Britain to maintain most of its pre-COVID ‘normality’.
Advocates of this approach are quite correct to underline the seriousness of the ongoing public health emergency, even with a vaccine, against the now somewhat quieter voices urging an immediate end to all restrictions. But it is less clear that ‘zero COVID’ can be treated as a long-term strategy to deal with the disease.
Elements of a zero-COVID strategy
The demand for zero COVID rightly sets a high bar for the current lockdown conditions, insisting on working towards the virtual elimination of COVID in Britain. It is critical that, unlike the experience last year, lockdown is not ended too soon. Aiming not only to “protect the NHS”, as is still the aim of government, but to reduce infections to near-zero would place this country (like any other) in a far better place, post-lockdown, than it was in following the first or second lockdown. It is also undeniable that the countries that went in hard against the virus early on, have been reaping the benefits – from Vietnam and Taiwan to New Zealand and Australia.
But it would be a major error to think that zero COVID is a permanent solution to the crisis we are now in. The Left and progressives absolutely must not become enthusiasts for lockdown: it is a terrible necessity, not some desirable point to get to. We should no more be cheering for this than we would cheer for war – a war may well be necessary at some point, but it’s hardly something to be called for gladly. The fact is that we have a terrible disease to deal with, and have to do so in a way that minimises death and illness from the disease – but also, importantly, from how we deal with the disease.
The cost of lockdowns is high: not because Gross Domestic Product takes a knock, or because the government has to borrow money, but because of the strains on mental health, on children’s education, or in the sharp rise in reported domestic violence cases. We should aim to minimise the costs of COVID, but we then need to also minimise the costs of lockdown. This means looking to leave this lockdown at an appropriate point, and acting now to never return to lockdown again.
We still have the option, with an effective suppression strategy, of getting to a very low rate of infection – although there is some uncertainty about what ‘very low’ should be defined as. But we must be serious about what achieving this means in practice. As Professor Sridhar has highlighted, it means three key things.
Firstly, it means comprehensive financial support, preferably in the form of unconditional cash payments to all – taxable later for those that can afford it. This is the easy part. No one on the Left would have much problem with saying benefits should be universally available.
It also means a comprehensive test-and-trace system. This is a bit harder for those of us who care about personal freedom. Successful contact tracing requires a degree of intrusion on people’s lives that is beyond the point we would have tolerated, pre-pandemic. It needs human contact-tracing to winkle out some of those details of where someone has been, and with whom. Human contact-tracing has been critical to the success of Vietnam and South Korea, for example. The various apps now in use around the globe, including in the UK, are not enough, as experts warned before their rollout last year. Either way, some intrusion, data collection, and data retention is required to make the system work.
But, categorically, zero COVID means a firm border-control regime. It is not serious to pretend otherwise. If the aim is elimination, then sources of virus transmission must be removed. Hard domestic social distancing, backed up by testing and contact tracing, reduces the chances of domestic outbreaks. Tight controls on the movement of people in and out of a country have a similar impact on transmission arriving from elsewhere.
Every country in the world presently held up as a successful example to follow currently has very tight controls on entry for people. There is no other plausible route to preventing the virus arriving from the rest of the world. Either you accept this, or you do not.
A short-term solution to a long-term problem
But this opens up the two major problems with zero COVID as any sort of long-term goal. To understand this, it is necessary to shift the frame of how we think about COVID from the national context, where a zero-COVID policy is expected to operate, to the global. All human diseases have a history that is shaped by the society around them, which in turn shapes the evolution of the disease. To understand their impact, we need to think about both the disease, and the human societies it exists in.
Malaria predates modern humans, emerging 100 to 200 million years ago and moving to infect our ancestors in the tropics, restricting the growth of human habitats where it is prevalent. Smallpox most likely appeared in east Africa some 3-4,000 years ago, following animal domestication and the invention of agriculture. Its arrival with the conquistadors in the Americas, where no immunity existed, assisted the destruction there of whole civilisations. The second-known bubonic plague pandemic, Medieval Europe’s Black Death, saw the Y. pestis bacteria carried into Europe through the greater trade and mobility that the Mongol Empire established. Its sheer destructiveness – killing one in three of the European population – fundamentally weakened the structures of feudal society and cleared the path towards capitalism.
COVID-19 also emerged at a specific point in our history. It has spread because of how we organise ourselves, and the path the pandemic takes from here onwards will depend on that social organisation. The biological features of the disease – critically, its respiratory transmission, its long period of dormancy, and the high number of asymptomatic cases – play into how we organise our society in crucial ways, and account for its rapid spread. COVID is, in other words, a disease of capitalism, and it is in this register that it is best understood.
To understand the course of the disease, we have to understand how it relates to the global capitalist economy we all live in. We can take this understanding in two parts.
The biological parameters of COVID-19
It is only a little over a year since the SARS-Cov-2 virus that causes COVID-19 was identified. Progress in both understanding how it behaves, from its genetics to its epidemiology, has been extraordinarily rapid, as has the development of effective vaccines. This gives a little more confidence to future forecasts as the progress of the disease; we are still peering into the murk, and know very little about its long-term impacts – crucially on long-term immunity from vaccination, and the effect of vaccination on the transmission of the virus. But it is possible to at least get some understanding of where we might get to.
A broad consensus has emerged amongst epidemiologists that, subject to some uncertainties, the most likely future for COVID is that it becomes an endemic disease – something that circulates within the human population for years to come, with the risk of occasional outbreaks. There is a high degree of uncertainty about what form that will take. However, the 100 or so experts surveyed by the science journal, Nature, were broadly optimistic that while COVID could be reduced in its severity, the prospects of a generalised eradication of COVID – as opposed to more limited, localized elimination, for example in specific countries – will be extremely difficult to achieve. On the most optimistic scenarios, and at least some of the early evidence from vaccines on severe disease points us towards them, we could over the next few years get to the point where the virus circulates – particularly in winter – but “we barely notice it”.
This perspective on the future course of the virus is informed by experience. We have eradicated only one human virus in the wild – smallpox, which was officially declared extinct in 1980, just over 200 years after Edward Jenner introduced the smallpox vaccine. Meanwhile, plans to eradicate diseases like polio on the basis of vaccination have significantly reduced its presence, but it remains endemic in key locations and the programme has faltered at the ‘last mile’. Political instability and the circulation of mutations of the virus have proved insurmountable.
Eradication is extremely difficult, and no serious plan for zero COVID focuses on it. However, elimination – reducing outbreaks of the disease to a minimum over a given period of time – is also very unlikely. Because COVID is a respiratory illness with a long period between infection and the first symptoms appearing (where they appear at all), it will be fiendishly difficult to remove from the whole population, as the historian Mike Haynes has argued. The economic costs, as with other respiratory diseases, of attempting to do so rise very rapidly the closer the disease is to being eliminated. One recent paper attempts to model for its progress over the next few years using what we know about both SARS-Cov-2 and the six other respiratory coronaviruses known to infect humans. Assuming it behaves similarly to the four coronaviruses in wide circulation – which we suffer very frequently from when young, usually as an unpleasant cough or sniffle, and from which we gain a long-lasting immune response – the modelling suggests we would move towards an endemic version of COVID over the next decade or so, in concert with social distancing in the early phase of the pandemic, and continued vaccination.
Most optimistically, a concerted vaccination programme rolling-out now might, in the future, leave us with a very much milder version of the disease, infecting the young and granting them long-lasting immunity, without the need for a permanent, rolling programme of vaccination. The key assumption here is that SARS-Cov-2, if contracted when young, would, like other human coronaviruses, lead to at least some long-term immunity and over time would become “no more virulent than the common cold”.
This is, necessarily, speculation that is informed by a model. Importantly, it does not account for the real way that human society is organised: it assumes one big planet that we all live on, not a planet divided into different countries with competing firms – the actual world of capitalism that we inhabit. But the modelling does start to establish the range of what we might plausibly expect in the next ten years or so. Importantly, it does not lead us to expect an eradication of COVID-19, even with vaccines.
What the modelling forecast points towards is the prospect of an eventual future where a relatively tame version of COVID is in circulation, but its management is not something that imposes exceptional demands on society, as it currently does. Plausibly, we could end up with a worse outcome: the kind of selection pressure being applied to SARS-Cov-2 via vaccination could, for instance, lead to the selection of viruses that are more transmissible and, potentially, more destructive in their effects. (The idea that viruses steadily become less aggressive over time is, unfortunately, something of a Victorian hangover. Dengue fever, for example, has become more virulent in the last 50 years or so, even as it becomes more widespread.)
It is not too hard to envisage a variant of COVID-19 emerging that was far more severe in its impact amongst the young, for example. The model in the paper gives us a relatively optimistic version of what could happen in the future, based on its assumptions. The key takeaways are twofold. Firstly, even a relatively optimistic scenario is very unlikely to include the eradication or elimination of SARS-Cov-2. And secondly, it is the transition to an endemic future point that should be our main point of concern. We need to think about COVID-19 as a relatively long-term problem, rather than something that can be dealt with as a short, sharp shock.
We are already seeing the emergence of virus variants with some evolutionary advantages against vaccines. The problem here is that a partially vaccinated population, with at least some people immune to the most-circulated strains of the virus, creates pressure on the environment the virus needs to thrive. That means that whilst strains of the virus that the vaccine promotes immunity to will generally find it harder to spread, the space remains open for mutations that are vaccine-resistant to then flourish. Vaccination has to be quick and comprehensive to get ahead of this, and in credit to the NHS vaccination programme, that is currently happening in Britain.
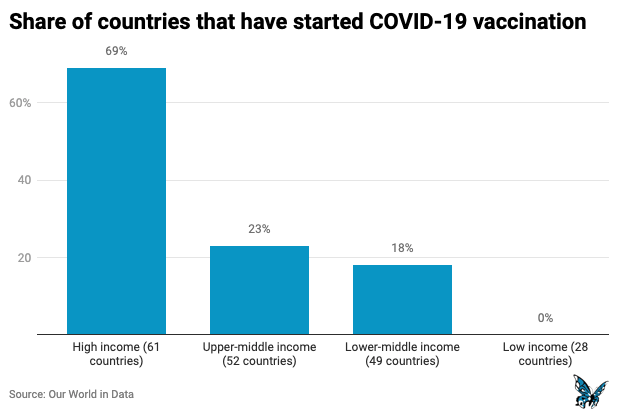
What it can’t guarantee is that this will happen elsewhere. We’ve already seen ugly eruptions of ‘vaccine nationalism’, as different countries compete over access to the limited resource of available vaccines. Developed countries have hoarded available and future supplies whilst the roll-out in poorer countries is expected to take far longer. The pattern, across the world, is likely to be of fairly patchy roll-out as countries compete over available stocks, made worse by likely future mutations in the virus itself.
This indicates the essential requirement to vaccinate quickly and thoroughly, but also that the period over the next few years, approaching a stable, endemic point, will not involve a simple return to pre-COVID ‘normality’ for most the population – as the activists around the Great Barrington Declaration have urged. We can’t do the equivalent of closing our eyes and pretending this will go away by itself. Policy and planning matter.
The political economy of the pandemic
It is not unreasonable to claim that elimination, globally, should be the aim of governments. In principle, we now have both the policy – zero COVID – and, crucially, the technology – vaccination – that at least create this as a possibility. To reach it would require most, if not all, countries to apply zero COVID as their aim, and vaccines to be distributed smoothly and effectively, repeating doses as needed.
It’s certainly possible to imagine a world in which the vaccine has been distributed fairly and countries everywhere have implemented zero COVID. Unfortunately, this isn’t the world we live in. We live in a competitive global economy, with states working alongside their national firms to compete against other states and firms across the globe. Ours is a world in which the worldwide co-operation needed to achieve both generalised zero COVID and effective vaccination do not exist, and most likely achieving even one would be difficult. As the vaccine roll-out continues, and some countries begin to benefit from the immunity they provide, these sorts of tensions that have already appeared around the vaccination programme, like those between the UK and the EU, are likely to worsen and recur every time new vaccinations are required. Given the likelihood of mutations, this is likely to be often. The best expectation for the global vaccine roll-out is that it will be highly uneven.
Similarly, the major incentive for countries – particularly those like the UK that are tightly integrated into the world economy – to avoid the costs of zero COVID are significant, especially where those costs fall on major businesses. The costs today of a serious suppression strategy are both the domestic losses (both economic and social) from restrictions in our activity, and the losses from shutting borders to outside travel. The benefits of zero COVID implemented today start to appear in the future, as the virus is brought towards elimination at least on a national level. This makes the future benefits hard to achieve without a firm steer politically.
But the more the rest of the world moves towards eliminating the virus, the lower the future benefits of zero COVID start to appear: if the rest of the world is bringing the virus under control, why should a country take on the costs of doing so itself? In other words, the more other countries implement a zero-COVID plan, the less incentive there is for any given country to also implement one.
This applies even when the future benefits are clear to everyone. It’s obvious now that those countries that did best in the first phase of the pandemic are now reaping the rewards, with the economies of China, Vietnam, New Zealand and others forecast to grow relatively quickly over this year. Clearly, when the virus has exploded and the costs of failure to control it domestically are high, there is a solid incentive for any given country to do something – although even this isn’t guaranteed, as the case of the US in 2020 shows, or in the brief period of ‘taking it on the chin’ in Britain.
But as vaccines are rolled out and the virus is (unevenly) brought under more control globally, this ‘free rider’ problem – of countries trying to avoid the costs of elimination by relying on others to do the work – is likely to become more apparent. This is because as the virus is brought under control globally, the future benefits of elimination in any given country, relative to the general level of the virus globally, are reduced: the gap between having no virus domestically, and the situation in the rest of the world, will have been shrunk. The vaccine will be reducing cases domestically, and vaccination in the rest of the world will be reducing the likelihood of importing cases. The costs of zero COVID will look less and less appealing relative to a reduced future benefit.
At the very least, the domestic coalition needed to sustain political support for zero COVID – across different business sectors, and into wider society – is likely to fray, given the presence of those extended costs and the fact that businesses face a competitive global economy. If they can palm off costs, they will; it takes exceptional domestic political pressure to overcome this. The most likely outcome globally is that if even a few countries implemented zero COVID in the initial stages of the disease, over time fewer countries will do so. More likely will be messy combinations in various countries, across the globe, of some attempts at suppression followed by periods of reduced restriction.
Put these two factors together – the difficulties in vaccine distribution, and the costs relative to future benefits of zero COVID – and it should be clear that a capitalist world economy is going to undersupply vaccines where they are needed, and undersupply elimination policy across different countries. We may get lucky, but the most likely path in the future is a fairly rocky one towards something like endemic COVID, globally, as in the modelling discussed above. That means any country pursuing zero COVID today, complete with border controls, test and trace, and extensive financial support for those self-isolating, is likely to have to do so for a significant period of time: in effect, holding out against global capitalism and its endemic disease. If the costs are high, and the future benefits are declining, it will become increasingly hard to hold the line. In New Zealand, repeated lockdowns from outbreaks are prompting debate about the long-term future of its own zero-Covid strategy: it is unlikely, given the global picture, that its current course will be maintained indefinitely.
Tight border controls might be bearable as a temporary measure, and command widespread public support in the UK. What we don’t know is how long they can be sustained at the kinds of levels that an elimination strategy would require. Take New Zealand as a much-cited example: since March last year, its border regime has become strikingly draconian. Only residents and their partners are allowed to enter, with visas to others being granted in only an exceptional number of cases. Asylum obligations have been suspended. Family returns are extremely limited. Cases of legal New Zealand residents becoming stranded by the border regime have emerged. The costs, in a crude economic sense, of severely restricting the flow of people in and out of a country are significant – particularly so in an economy like Britain’s. But there is also the slow social damage of attempting to maintain yourself as a weird semi-autarky for an extended period of time, or of attempting to maintain extended periods of enforced social distancing.
Fences and passports
Proposals to try and ease the costs of an extended period of suppression are already starting to emerge. Immunity passports indicating a person’s current vaccination status and therefore their eligibility to travel, have been floated by the former UK prime minister, Tony Blair, whilst the European Commission has just proposed the introduction of a digital vaccine passport for holidaymakers inside the EU this summer. We are seeing the emergence already of ‘travel corridors’ and ‘approved lists’ of countries, and hard travel bans on others. It is not too hard to imagine a world in which the distribution of vaccines is limited in effect to a relatively privileged minority, who are then biologically cocooned from the wider world in a system of travel corridors and vaccine passports. This would leave the world’s majority patchily vaccinated, suffering repeated waves of fresh mutations of the virus and trapped behind new fences along the rich world’s borders. This is not too hard to imagine as a near-future because, of course, this is very similar to the world we already live in.
Importantly, zero COVID could very easily fit in with a world that starts to look like this: countries that agree amongst themselves that they have eliminated the virus could decide their citizens were allowed to travel amongst themselves, whilst maintaining tight restrictions on entry to the rest of the world. Australia and New Zealand have already made exactly this agreement. In the place of what historian Le Roy Ladurie, surveying the devastation of the Americas, called the “unification of the world by disease”, COVID looks set to provoke its further disintegration.
[slide-anything id=’3472166′]
The likely outcome of attempting to deal with handling the virus at the level of the nation state is therefore to reinforce some of the most discriminatory aspects of the state itself: either more authoritarian at home, or more exclusionary towards the rest of the world (or, of course, both at once). A world beginning to be structured like this, with cocoons of relative success in handling the virus holding out against the failures, would reinforce the tendencies we have seen since 2008, as so much of the pandemic already has: towards greater inequality, greater state involvement in the economy, the reordering of the global trading and commerce system, and (if some of the various proposed biosecurity measures are introduced), greater digitisation of social and economic life, notably at border crossings. It is not in any sense a desirable version of the near future.
Alternatives
Where does this leave us? Fundamentally, that the scale at which we think about the crisis must match the scale of the crisis itself. The nation state cannot be the start and end point of our thinking about solutions. Instead, we must try to think in two directions: firstly, to the global structures of capitalism that SARS-Cov-2 has very successfully leeched off, with ourselves as the unfortunate vectors for its spread; and then secondly back towards the micro-level scale at which transmission takes place, in the ways in which relate and interact with each other.
We need to revise our time horizons, too, and plan for a longer period of transition towards a more stable situation with the disease, looking beyond immediate crisis responses. The UK government has floated an “endemic recovery plan” of five to ten years’ duration, and this is the kind of timescale we should all be thinking on given what we now know about the disease. But if that is the case, it is too long a period to plausibly suspend social life for, or to lurch between lockdowns and releases. Instead, we need to think of the ways in which we can fairly adapt how we live and work in order that we can maintain what we most enjoy about life. If the primary aim remains, for the foreseeable future, to bring down the number of social contacts we have, priority should be given to the contact we appreciate most – meeting friends and family, attending public events – and limiting what we tend to dislike – work and commuting. If the duration of the pandemic is extended, this should be treated as a design issue, rather than a policing problem.
What might a programme for a just transition – if we can call it that – beyond zero COVID look like in practice?
Firstly, it means delivering the most rapid distribution of vaccines globally that can be technically achieved on the basis of need, regardless of national origin. This means not only releasing the stockpiles (or future stockpiles) that have appeared in the developed world, but overriding the intellectual property regime where it constraints the most rapid production and distribution possible, as the South African and Indian governments have requested.
Second, it means creating slack inside national healthcare systems to cope with future outbreaks, and the integration of social and childcare into the broader system of care. All such care should be made free and available at the point of need. Specific funding should also be allocated to ‘long COVID’, and the needs of its sufferers, who currently remain under-served by the allocation of emergency healthcare funding.
Third, it means strict limitations on the application of exceptional border controls, travel corridors, the use of vaccine passports, and any future such tool – with agreed, objective parameters and guidelines on their use and clear sunset clauses. These are ultimately illusory nation-state ‘solutions’ to a global problem.
Fourth, it means redesigning public spaces around the principles of allowing for greater social distancing: more space made available, at variable times of day, including the repurposing and refitting of commercial spaces like shops that are unlikely to survive the pandemic. For the developed world, this should include the redesign and repurposing of high streets away from high density commercial activity. Schools and other high-density educational institutions should be repurposed to a lower density of use. It could also include the creation of lower-density, reduced-travel urban areas, as for instance in the 15-minute or one-minute city proposals.
Finally, it means the reduction of working time and promotion of home-working as an effective means to reduce physical contact where this is possible. This is likely to include short-time working support and some form of universal basic income within an expanded welfare state provision. Necessary healthcare and other protections must also be provided in workplaces.
Some of this will involve a significant role for the state, out of necessity. Monitoring of the health situation will be an unavoidable necessity, but such monitoring and the data collection it involves must be subject to proper and transparent legal controls.
But our aim should be, as far as possible, to shift what the state does away from its repressive functions, and towards the provision of care. And where this involves an expansion of the state’s functions, the burden of costs must be placed on the broadest shoulders – in other words, a shift in the tax system. Much of this could fit very well with ambitious plans to decarbonise and otherwise reduce our environmental impacts: greater home-working, as we now know, reduces travel time, much reducing carbon emissions.
Could it go wrong? Of course. It’s impossible to guarantee that fresh mutations of the virus won’t be significantly worse than the strains currently circulating. They could be more transmissible, or with a different pattern of health impacts. Scenarios like this would involve a significant tightening of controls and social distancing. And with zoonoses – infectious diseases that jump from animals to humans – increasing, and clear evidence now emerging of the relationship between climate change and the emergence of new diseases, COVID-19 is highly unlikely to be the last such pandemic we face.
But if the principle is to build in a degree of resilience against COVID-19, that resilience will also hold for future, similar challenges. What we cannot do is assume that a short-term emergency proposal such as zero COVID is a substitute for the long-term changes that are needed.
Teaser photo credit: By Chairman of the Joint Chiefs of Staff from Washington D.C, United States – 201221-D-WD757-1126, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=97947808




