
 The discussions in the US this week surrounding the constitutionality of health insurance payment mandates and the fact that my terminal degree is in health policy helped me to choose a topic for this week’s post. The US Supreme Court question that the Justices are examining this week has to do with the issue of insurance payment mandates for individuals—is it constitutional? The goal of Obama’s The Affordable Care Act is a goal of healthcare for all within the existing system.
The discussions in the US this week surrounding the constitutionality of health insurance payment mandates and the fact that my terminal degree is in health policy helped me to choose a topic for this week’s post. The US Supreme Court question that the Justices are examining this week has to do with the issue of insurance payment mandates for individuals—is it constitutional? The goal of Obama’s The Affordable Care Act is a goal of healthcare for all within the existing system.
One primary argument of those supporting the plan is that, while not perfect, the plan is a good start in transitioning to a universal healthcare system. Yet the plan and the current discussions make a number of unstated assumptions about a healthcare system embedded within a capitalist, free market economic system of the wealthiest country on the planet. These assumptions need to be exposed in order to view the problem systemically. I would suggest that these assumptions are not even correct to begin with for the existing system, and that the assumptions will become even less true in a permanently declining economy associated with peak oil.
Rousseau said, “Good laws lead to the making of better ones; bad laws bring about worse.” In my opinion, creating bad laws now that assume that the current system can grow infinitely only lead to further catastrophe.

Flywheel from MT Brown 2004 Picture Worth a Thousand Words (from Odum, 1976)
Public policy is whatever governments choose to do or not do (Dye, 1995). Policy is the authoritative allocation of values for the whole society (Easton, 1975). Politics, then, is the act of how we get policy done. In our current western economies, policy resistance is occurring due to embedded vested interests of powerful corporate players in the policy arena. Reinforcing feedback loops (autocatalysis) creates an imbalanced system and dominance, which then creates more imbalance, eventually leading to a sort of super-circulation such as our exponentially growing flywheel economy.
As we expand the current healthcare system, autocatalysis causes an extreme super-circulation similar to that found in the economy at large. A market-based healthcare system gives the strongest shareholders the most power to garner even more profits (Kuttner; Hsiao, 1994; Arrow). A crowded policy environment with too many players creates gridlock, allowing only incremental expansion instead of significant needed reform. As in the economy at large, too many powerful vested interests create more inequity, more debt, and more consumption (treatment) with less regulation and more profit.
Meadows (2008) describes policy resistance as an attempt by various actors to pull a system stock towards various goals. “Any new policy, especially if it is effective, just pulls the stock farther from others’ goals and produced additional resistance, with a result that no one likes but that everyone expends considerable effort in maintaining” (Meadows, 2008, p. 116). Thus, defining the goals of the system and the assumptions embedded within those goals becomes critical. While the trigger for this post is American healthcare as the extreme case, some of the systemic issues can be applied to various sectors in other countries, too. The unstated assumptions regarding growth of any economic sector at this point in time need to be stated and examined from a systemic perspective. I would like to expose healthcare assumptions as an example du jour, using a framework of the traditional triad of health policy values: quality, access, and cost.
General Structural Assumptions/Goals of the Current U.S. Healthcare System
- Healthcare is a commercial commodity that can be developed and sold
- Healthcare can support profit while providing adequate care for all
- Healthcare allocation is unnecessary; rationing is effected by market costs
- Healthcare policy can continue its expansionary growth in the face of peak oil and economic contraction
- The current healthcare system (HCS) in the US is functional and is worth expanding
- The current level of bureaucracy and complexity can be incrementally expanded
- Insurance linked to employment works in low employment situations such as recessions as well as vibrant, high employment situations
- Just in time efficient healthcare is resilient to impacts of increased needs for healthcare
Quality Assumptions:
- The current HCS in the US is effective in promoting health, healing the sick, and prolonging quality life in the elderly
- The current HCS places the interests of patients as primary
- Insured patients receive the proper amount of care (not too much or too little treatment)
- Libertarian ethical emphasis on individual autonomy and personhood assume infinite capabilities of our healthcare system to expand and provide for all
Access Assumptions:
- Healthcare should be a right for all, whether we pay for it or not
- The US has the ability to incrementally expand the current system and support additional complexity and profit while meeting the needs for all

- There is no political or ethical need for restraint of healthcare
- The US has the ability to expand the healthcare and the economy in the future
- The US has the ability to provide infrastructure (hospitals, intensive care units, healthcare workers (HCW) to meet expanded demands from increased numbers (from healthcare reform and aging boomers) at the current level of intensity of care

Cost Assumptions:
- US healthcare is a mix of private, public, and mixed produers embedded within a capitalist economy, favoring private solutions wherever possible
- Debt and entitlements to the future ($200T?) do not matter
- Copayments for those with insurance are affordable

Ritholtz Big Picture
- Insurance attached to employment basis is a good way to provide insurance
- Health Insurance protects families from damaging economic consequences
- Healthcare AND Insurance markets are sound, competitive, efficient, and fair. Markets have:
- Enough competitors
- Pricing which affects producers and consumers
- Freedom of competitors to enter or leave market
- No collusion among competitors
- Informed choice for consumers (McClure, 1983)
Many of the assumptions stated above regarding American healthcare policy may not be supported by current realities. I rephrase the assumptions below from a larger systems perspective. Each one of these bullet points could probably be a post in itself, with many links, references, and supporting arguments. The goal here is simply to suggest a different world view.
Quality Realities:

- Marketization pursues efficiency and profit rather than quality (Hsiao, 1994)
- Insurance companies have a primary goal to provide profits for shareholders and to restrict costs to their companies
- Patients are overtreated (medicalization) in order to increase profits in a market system through supplier-induced demand
- Libertarian ethics redirects attention from utilitarian welfare and justice
- Much of the real gain in healthcare improvement has come from socioeconomic and public health improvements such as clean water, modern sewage systems and adequate healthy food (Frieden, 2010).
Access Realities:
- Policy changes to expand insurance mandates (rather than expanding basic healthcare for all) tailors the problem to existing assumptions of profit-based healthcare and infinite growth
- Consolidation and conversion from non-profit to for-profit of insurance and hospital systems have consolidated power and placed corporate profits before care

Logan, 1998 HC Policy Model Insurance Profits under Managed Care
Cost Realities:

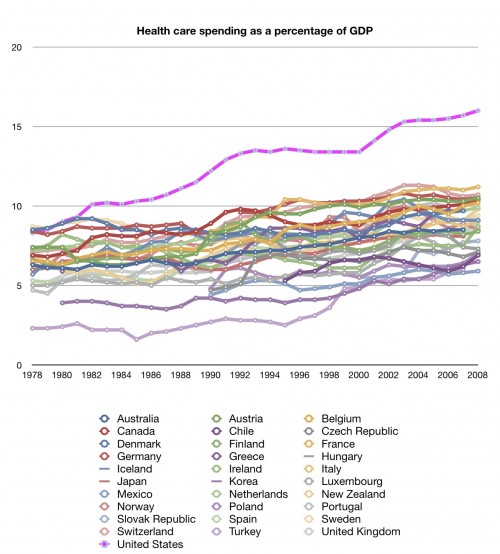
- US HCS currently costs twice that of most other developed countries, with lower quality. Demand side controls do not work; supply-side regulations are needed
- Over time insurance premiums have risen while coverage has trended down (Newsom & Fernandez, 2011, Congressional Research Service)
- High deductibles and copayments in a descending economy result in less treatment for patients and higher profits for insurance companies (NYT, 2011)
- Healthcare and insurance markets are inefficient, unfair, and monopolistic. In an analogy, if healthcare is a factory, patients are cogs in the hospital/clinic assembly line. The administrative bureaucracy is the floor manager. Physicians are customers, and the Insurance/Pharmaceutical Industry are the owners. Gatekeeping control of drugs and treatment is by profit-making Insurance and Pharmaceuticals
- Pricing is obscured or absent until after the fact (billing). Private market financing is inefficient due to risk-selection and high management costs
- Competitor entry into markets is limited by federal, state, and local laws for healthcare entities and a 15 year, exorbitantly expensive pipeline for physicians with strict quotas, heavy federal subsidies, and gatekeepers. Long pipelines require proactive interventions to avoid imbalance in the system
- Powerful healthcare and pharmaceutical lobbies act as collusion in markets by gaming the system and promoting favorable regulations
- Outcomes information for consumers is limited, obscured, or gamed in the media, creating imbalanced power between producers and patients
- Insurance is positioned at the front of the healthcare payment pipeline; they siphon off optimal profits with minimal regulations. “In the midst of a deep economic recession, America’s health insurance companies increased their profits by 56 percent in 2009, a year that saw 2.7 million people lose their private coverage” (Walker/HCAN, 2010, ABC).
- Monolithic healthcare entities’ size makes them powerful and relatively invulnerable to change
- Expanding the insurance mandate to all will create more healthcare consumers; then more healthcare will mean more profit for private insurance companies and increased strain on consumers and healthcare entitites such as hospitals and physicians
- Even with insurance, the cost of healthcare treatments can bankrupt families
Conclusions
Peak oil and diminishing resources are linked to a cessation of economic growth and hence to economic contraction. In the future, our advanced, technological western healthcare system will arguably need to contract in complexity, size, and profits, as we have less resources available to spare within economies. Permanent economic contraction will lead to disappearing traditional corporate jobs, and thus disappearing traditional health insurance linked to those jobs. At the same time, diminishing resources will lead to inflation in all sectors including healthcare, and decreased ability for insurance companies to provide adequate payment and decreasing ability of consumers to pay for insurance. Stressors in the economy (including pollution buildup) will lead to decreased health and increased pressure on healthcare.
Hierarchy and autocatalysis drives the complexity of our healthcare system. Our complex society focuses costly interventions at the top of the hierarchy while taking for granted the socioeconomic benefits derived from our fossil fuel slaves, which are only present as long as the fossil fuels are present. At the same time, effects of surplus consumption and surplus wastes also impact our health, creating more problems with each loop of the economic engine. Our HCS is another imbalanced hierarchy; top heavy with complexity and too much treatment for too few and not enough treatment for the rest.
The rise in the number of people being treated for expensive conditions has had an impact on the growth in private insurance spending similar to that on overall health care spending. The rise in the number of people being treated, rather than the rise in spending per treated case, was the most important determinant of the growth in private insurance spending between 1987 and 2002, according to a recent study. For 16 of the 20 most expensive conditions, the rise in the number of people being treated accounted for more than half the growth in private insurance health care spending. Researchers attribute the additional numbers of people being treated to three factors:
- The continued rise in the share of privately insured adults classified as obese.
- Changes in clinical treatment guidelines and standards for treating patients without symptoms or with mild symptoms only.
- The availability of new medical technologies to diagnose and treat patients.
Especially important is the increase in the number of people treated for conditions clinically linked to obesity. From 1987 to 2002, the proportion of the population treated increased 64 percent for diabetes (accounting for 80 percent of the increase in costs) and increased 500 percent for hyperlipidemia (accounting for almost 90 percent of the increase in costs). A number of factors might explain the substantial increase in treatment rates for conditions linked to obesity. These factors include a rise in the number of people with obesity-related conditions, a rise in the number of more seriously ill patients, a greater emphasis on preventive care, and the introduction of broader treatment options (Stanton, AHRQ, 2006).
In a crumbling economy and healthcare system, maintaining or expanding spending for chronic conditions, especially in the very aged, is an unsustainable trap. Similar to any other part of the economy, our fossil-fuel based lifestyle has allowed us to leapfrog past basic needs and focus on the wants at the higher levels of the complexity pyramid instead.

TRFriedenApril 2010, 100(4)Am Jo Public Health
The most bang for our healthcare buck occurs in providing improvements in socioeconomic factors–preventive, systemic changes that result in improved quality of life. Those changes have occurred naturally over the past two centuries as a function of fossil fuel related improvements in public health and complexity. (See also Hans Rosling’s 4 minute Gapminder video on “200 years that changed the world.) Yet most of our current healthcare interventions occur at the top of the pyramid above, in costly, high-tech clinical interventions. If fossil fuels are constrained in the system, then both the top and the bottom of the healthcare hierarchy become disordered, requiring change. Healthcare is one of the last bubbles in the US economy. We need new goals and a new healthcare system that is focused on justice and the good of the whole, rather than profits and personal freedom.
The most effective way of dealing with policy resistance is to find a way of aligning the various goals of the subsystems, usually by providing an overarching goal that allows all actors to break out of their bounded rationality. If everyone can work harmoniously toward the same outcome (if all feedback loops are serving the same goal) the results can be amazing. The most familiar examples of this harmonization of goals are mobilizations of economies during wartime, or recovery after war or natural disaster (Meadows, 2008, p. 115).

A permanently contracting economy will result in a bioethical crisis as fewer resources are available to an increasingly stressed global population. We need to reconsider our goals of expansion of capitalism-driven wealth as the system loses its surplus energy. Instead we need to consider the sustainable good of the entire country during the contraction of the economy. We need justice in terms of basic needs for all, with more attention to the health of entire communities rather than individual rights. Failure to provide basic needs for all affects the whole system, with increases in epidemics due to stress, overcrowding, poor nutrition, dirty water and pollution, and failures in vaccination programs and general control of illnesses.
Based on the apparent politics of today, as we continue to descend, what we will probably get as the system becomes more imbalanced and unsustainable is limited fee for service care for the wealthy (with eventual failure of insurance), very limited care for the poor, and early mortality for many. Perhaps Obama’s healthcare proposal is the only politically feasible step in our currently gridlocked and imbalanced policy arena. But if we potentiate the power of Big Insurance and Big Pharma with healthcare reform that reinforces feedback to them through increased profits, aren’t we just one step further on the road to Too Big To Fail Yet Too Big to Sustain?





{kind=link}